The topic of carpal tunnel surgery keeps coming up in my Facebook news feed. Both in my pole and aerial feeds and in my friend groups. I read the comments and think about writing a dissertation on the topic in the comments as I know way more about this than the average bear. (oh, wait…I kinda already did write a dissertation on it during that whole PhD thing….) So this is my blog post about it….
Here’s the deal, I’m PhD researcher that studied upper musculoskeletal disorders in musicians. AKA arm pain, shoulder pain and all the cool things we name it like carpal tunnel. After falling in love with Pole and leaving the musician injury field I now apply that knowledge to pole and aerial. I am not a medical doctors, so please insert the mandatory “consult your medical practitioner before doing anything I recommend” here.
What I’m about to say is controversial but supported by my extensive research. 2/3 of all carpal tunnel surgeries are not necessary. (I personally would put this figure even higher, but I’ll stick with the research supported figure.) A “true” carpal tunnel is when the space in the wrist is physically too small for the nerve. For most “true” cases this onsets very early in life and symptoms present very early. This is super rare, in my opinion. What we see in adult onset cases is that all the symptoms of carpal tunnel present (the pain is real!) but that the tunnel isn’t too small, the tunnel has just collapsed due to body compensations and years of use. Think of a train tunnel; the engineers built the tunnel big enough for a train (your nerve) to go through but then a rockslide happens and now the tunnel has obstruction. In many cases the person has surgery to make the tunnel bigger (but it wasn’t actually engineered wrong in the first place) and the symptoms get better for a short time, but then whatever was structurally causing the collapse before is still present and causes the new bigger tunnel to also collapse and symptoms return.
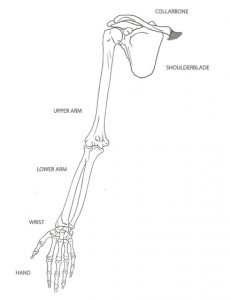 The most common cause for “tunnel collapse” that I’ve seen is the body compensating for a problem further up the arm at the wrist. The arm is very complicated. There are multiple points of movement, bend, rotation, and two very important nerves that run through the whole thing. If there is an obstruction anywhere along the nerve path you can feel it anywhere else on the nerve path. Most often, the pain refers to the wrist, even if the problem is higher up. When you look at the arm you can see there are two bones in the lower arm. These two bones have to pivot over each other any time you rotate your wrist. If these two bones stop moving “correctly” or freely over each other they put stress on either the elbow or the wrist or both. In many cases, it is the incorrect movement of the two forearm bones that create the carpal tunnel symptoms.
The most common cause for “tunnel collapse” that I’ve seen is the body compensating for a problem further up the arm at the wrist. The arm is very complicated. There are multiple points of movement, bend, rotation, and two very important nerves that run through the whole thing. If there is an obstruction anywhere along the nerve path you can feel it anywhere else on the nerve path. Most often, the pain refers to the wrist, even if the problem is higher up. When you look at the arm you can see there are two bones in the lower arm. These two bones have to pivot over each other any time you rotate your wrist. If these two bones stop moving “correctly” or freely over each other they put stress on either the elbow or the wrist or both. In many cases, it is the incorrect movement of the two forearm bones that create the carpal tunnel symptoms.
There are many ways to facilitate better forearm function.
- See a manual therapist. This is someone who works with soft tissue and bone and manipulates it back into a correct use pattern. Basically this person will find the compensations patterns your body has created to keep moving and will reverse them. If you are near Appleton, Wisconsin, go see Brennan Hussey, PT at 920-284-3048. He’s the best I know, anywhere. I’ve sent people all over the country to him.
- See a massage therapist and have them work a lot on the tissue by the elbows. To me this is a maintenance thing. It likely won’t solve the problem alone but once your pain is gone it is good to do this frequently so it stays away.
- Stretch your nerve pathways daily. Multiple times. There are two stretches that I think are key to alleviate forearm and wrist pain. Do both of these on both arms, even if symptoms are only in one. ONE arm at a time. Hold each for 10-15 seconds. Because these are nerve “stretches” and not muscular you can do them without warming up. You should do them after any pole or aerial work, whenever you use a computer or play piano, and in general every hour until you are symptom free. You can do these sitting or standing. Make sure the hand is at the side and not out in front or behind your body.

 Left Picture: Nerve Pathway 1
Left Picture: Nerve Pathway 1
Start Palm facing forward
Extend wrist back so palm faces floor
Drop shoulder down if need more
Drop head to opposite side if need more
Right Picture: Never Pathway 2
Palm facing back ball
Extend wrist up so palm faces ceiling, “grab your own wrist”
Drop shoulder down if need more
Drop head to opposite side if need more
Depending on your body you may only need to drop your shoulder or drop your head. If you get numbness or tingling, then extend your wrist back less and do more with the shoulder and head.
In my research carpal tunnel was treatable in all cases. It sometimes took time to sort out what worked but a solution was possible that was non-surgical. It’s important to note that computer use is one of the main believed causes of this type of wrist pain. Also important to note that many of the exercises people do to help wrist pain, like extending your arm in front of you and pulling on the hand, are actually extremely unhealthy for the wrist. A few tips:
- ALWAYS stretch wrists one at a time. Your wrists have different flexibilities so trying to stretch them together is not beneficial to either as one will be over stretched and one will be under.
- Never yank on your hand to stretch your wrist or forearm, this puts stress on areas that don’t need it. If you want something to push against use the wall or floor for even pressure.
- Whenever you do any elbow stand or elbow plank your forearms should be FLAT on the ground with your palms down, NOT on the side of the forearm! This is the safest position for your arm and wrist from a weight distribution and stress factor.
- Do self massage of your forearm a LOT. I like using a small one-inch rubber bouncy ball for this. Roll your forearm around on it making sure to get up around the elbow, both sides of it!
Hopefully this gives you hope that your wrist pain isn’t surgical! Instead, let’s work on forearm health to alleviate wrist pain!